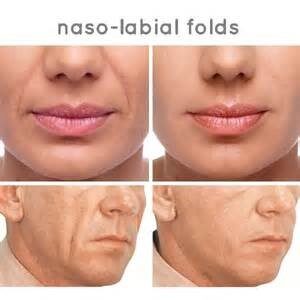
Nasolabial Folds
Nasolabial Fold & Marionette Lines (Nose to mouth & Puppet lines)
Safety with Nose to Mouth Lines – Treating this area of a client’s face is a safe procedure if anatomical particulars & safe anatomy is understood. When treating the nasolabial fold, it is important to understand how to prevent, recognise and treat the rare and serious complication of impending alar necrosis
Anatomy
A nasolabial fold is not always an age-related problem, it is often present even from birth, but it does become longer, deeper and acquire creases with age and accompanying volume loss and skin laxity. The deepening shadow is one of the primary unconscious indicators of the ageing mid face, and therefore also one of the easiest ways to rejuvenate the mid face. During smiling the action of zygomatic muscles highlights the fold, and over time this also has an impact on the surface of the skin where creases appear. It is common to see volume loss with overlying creases. The fold should become deeper during a smile, and over treatment that reduces this too much can cause an unnatural appearance. The deepest portion of the shadow is usually just inferior to the alar junction, and at this point a small shadow is normal. Obliteration of this shadow can make the nose look almost ‘stuck on’ rather than integrated into the face. Volume loss directly under the line and in the cheek above are the primary targets for dermal filler restoration
Awareness of the lateral nasal artery branching from the angular artery is important. Dermal filler placement near this artery can either compress the vessel, or if injected inadvertently intraluminal it will cause necrosis.
SEE DIAGRAM BELOW

Surface Anatomy
Examine the length and depth of the wrinkle and for superficial creases as well as volume loss. Treat the two features with an appropriate technique. Covered within you practical training
What Causes Them?
- Volume loss of the skin in general.
- Volume loss of the malar fat pat in the cheek.
- Slippage of the malar fat pad (more common in long distance runners).
- Increased skin laxity due to age and photo damage.
- Rapid or significant weight loss (commonly after gastric bypass)
- Genetics
- Also, serious disease such as HIV/AIDS.
Your safety as a practitioner.
In practice you should assume there are arteries under every injection point always check for a flash back by utilising aspiration.
Choice of filler to use;
Medium thickness fillers like Juvéderm 3 or Revolax Deep
Fine thickness fillers like Juvederm 2 can be used for surface creases in the same areas & are ideal for cross hatching in the mid face for volume loss.
Common mistakes
- Underfilling Being clear during your consultation is important – “1 syringe will make a significant difference, but you might need more to be completely satisfied”
- Not pointing out existing unevenness/asymmetry: The nasolabial line is nearly always worse on one side than the other, often a person will use one side of their face more for expression & therefore the muscles will be more established resulting in the creation of a more pronounced line. In addition, the side the client sleeps on can often appear deeper, due to more movement and pressure on one side of the face
- The client often will have not noticed this themselves but will be paying much more attention after their treatment. They may return suggesting you have not treated them evenly. Verbalise and photograph. Never promise to correct asymmetry – improve yes, but it may never be completely perfect due to characteristics of their natural anatomy
- Injecting filler above the nasolabial line- If the needle tip passes above the ‘valley floor’ of the line and filler is placed above the line the fold will appear worse- needs a firm downward massage to correct. This is probably a risk for damage to the angular artery too.
